The need for vitamin B12 and iron supplements is even higher after a Biliopancreatic Diversion, compared to other procedures, because of the malabsorptive nature of this operation type. After BPD/DS, the absorption of nutrients is very limited due to the large section of the small intestine that is bypassed. Absorption of fats is limited to the last centimetres. The “common channel” is reduced to such an extent that absorption of fats is disrupted. An extra high dose of vitamins A, D, E and K is essential to meet requirements.
Studies have shown that despite supplementation, severe deficiencies in vitamins and minerals exist after a BPD or DS. Anaemia, iron deficiency and deficiencies in fat soluble vitamins are often encountered. Regular monitoring is essential to identify deficiencies at an early stage. Taking everything into account, a strict programme of vitamin supplementation should be established.
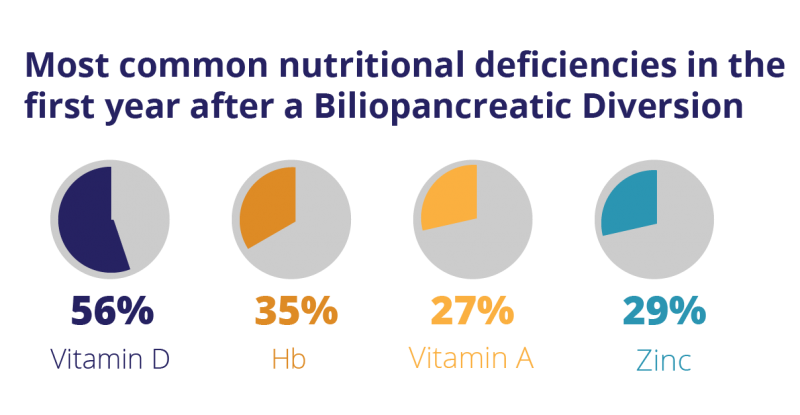
Deficiencies after a Biliopancreatic Diversion
Nutritional deficiencies after Biliopancreatic Diversion or Duodenal Switch were studied by Dr. Homan and colleagues. Results of this study show that the most common deficiencies after this type of surgery are vitamin D, zinc, iron and vitamin A. For BPD or DS patients, exceptionally high doses of certain nutrients are recommended in order to prevent or manage deficiencies.
The role of WLS Maximum
The high risk of developing nutritional deficiencies after a Biliopancreatic Diversion or Duodenal Switch clearly shows the necessity for a food supplement, tailored to the specific nutritional needs after this operation type.
Research has shown that within 3 years after a Biliopancreatic Diversion (BPD) or BPD with Duodenal Switch (BPD/DS), up to 90% of all patients develop nutritional deficiencies. For these patients, we have developed WLS Maximum. This product has recently been optimized to further support their elevated nutritional needs. The dosages of several nutrients have been increased. Other dosages were reduced, where we learned that the earlier levels were, although completely safe, higher than necessary.